

Your receptionist picks up the phone. A client describes their dog vomiting blood at 11pm. The receptionist knows this sounds serious but doesn't know if they should recommend emergency care, schedule tomorrow morning, or transfer to a vet. They hesitate, give vague advice about monitoring symptoms, and the client hangs up confused.
Three hours later, the dog arrives at emergency in critical condition. The client claims your clinic downplayed the urgency. Your insurance carrier starts asking questions about your teletriage protocols.
This scenario plays out constantly in veterinary clinics. Not because staff don't care, but because most clinics lack structured teletriage systems. Without clear scripts and decision thresholds, every phone interaction becomes a liability minefield where well-meaning staff make inconsistent recommendations that expose the practice.
The gap between phone advice and VCPR requirements
Most veterinary practices handle teletriage reactively. A receptionist answers, tries to gauge severity based on their experience, maybe checks with a tech if one's available, then gives their best guess at advice. Sometimes they nail it. Sometimes they send non-emergencies to ER at 2am. Sometimes they tell clients to wait when immediate care was needed.
The Veterinary-Client-Patient-Relationship (VCPR) creates strict boundaries around what constitutes legitimate medical advice versus general guidance. Cross that line without proper documentation and you're practicing veterinary medicine without an established relationship. Stay too conservative and you're turning away clients who need help.
Between these boundaries sits a massive operational challenge: how do you systematically triage cases over the phone while staying within legal limits and providing consistent client service?
Effective teletriage recognizes that not all symptoms require the same response pathway. Different symptom presentations demand different urgency levels. These categories form the backbone of your triage system.
Building decision trees that protect both patients and practice
Immediate emergency referral triggers include respiratory distress (open-mouth breathing in cats, sustained respiratory rate over 40 in dogs), pale or blue gums, inability to urinate (especially male cats), active seizures lasting over 3 minutes, uncontrolled bleeding, suspected toxin ingestion within 2 hours, eye injuries with visible damage, and bloated abdomen with unproductive retching.
Never miss a pet’s appointment again.
Veterinaryly helps you schedule, confirm, and manage every appointment and patient record effortlessly.
- Centralized appointment & patient management
- Automated client reminders
- Staff scheduling & task tracking
No credit card required
Same-day evaluation triggers include vomiting more than 3 times in 12 hours, diarrhea with blood, lameness with no weight bearing, facial swelling, excessive drooling with pawing at mouth, and not eating for 24+ hours in cats or 48+ hours in dogs.
Next-day scheduling is appropriate for mild lameness with weight bearing, single episode vomiting with normal behavior, ear scratching/head shaking, minor wounds without active bleeding, and mild diarrhea without other symptoms.
These categories need to translate into actual scripts your team can follow. The gap between knowing what's urgent and communicating it consistently over the phone is where most practices struggle.
Reception scripts that gather critical information fast
Receptionists need structured questions that extract essential triage information without requiring medical knowledge. The best scripts follow a specific flow that builds understanding progressively.
Initial assessment starts with: "I understand you're concerned about [pet name]. To help determine the best way to assist you, I need to ask a few quick questions. First, is [pet name] currently having any difficulty breathing, seizures, or uncontrolled bleeding?"
If yes, you move to immediate emergency referral protocol. If no, you continue assessment with "When did you first notice these symptoms?" followed by questions about walking normally, last eating and drinking, and any changes to urination and bowel movements.
This opening sequence immediately identifies life-threatening emergencies while gathering baseline information for less critical cases. The questions avoid medical terminology and focus on observable behaviors.
Severity assessment questions vary by symptom. For vomiting, ask how many times today, what the vomit looks like (food, liquid, foam, or blood), if they're keeping water down, and if their belly is bloated or painful to touch. For diarrhea, ask about frequency, any blood or black tar-like appearance, straining, and accompanying vomiting.
For trauma, ask about active bleeding, weight bearing on all legs, swelling around the injury, and whether they witnessed what happened. These questions help receptionists gather specific details without interpreting symptoms themselves.
Here's a simple workflow visualization.
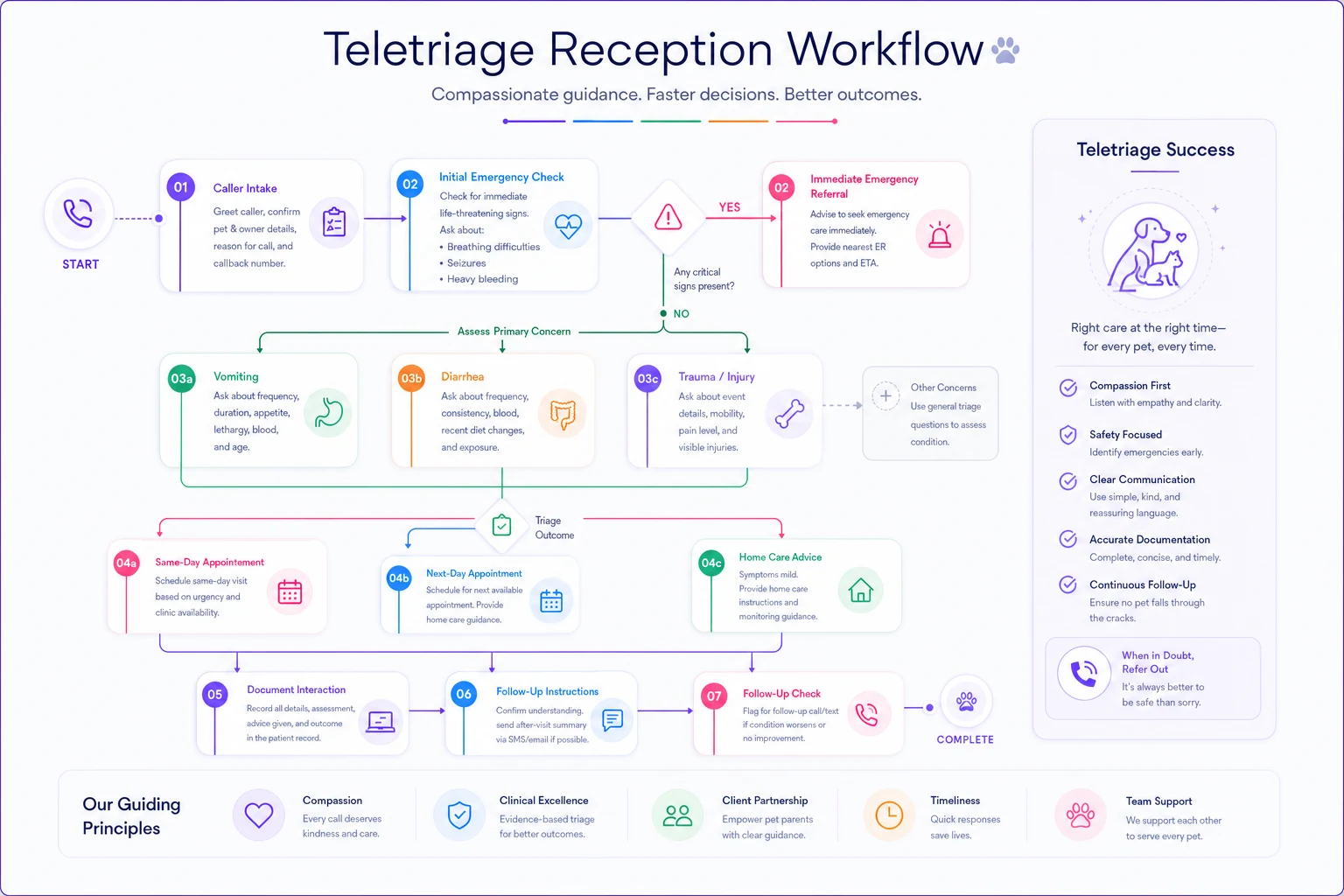
This opening flow ensures critical emergencies are caught immediately while collecting enough detail for non-emergencies.
Documentation templates that satisfy liability requirements
Every teletriage interaction needs documentation that protects your practice while providing continuity of care. You need templates comprehensive enough for legal protection but simple enough for busy staff to complete consistently.
Essential documentation elements include call timestamp and duration, client name and patient ID, presenting complaint in client's words, questions asked (checkbox format works well), symptoms reported by owner, recommendation given, whether client accepted recommendation, and staff member handling call.
A practical template would include date/time, client and patient names, call handler, chief complaint in owner's words, symptom checkboxes for vomiting, diarrhea, not eating, lethargy, breathing difficulty, urination changes, behavioral changes, trauma/wound, and other options with frequencies and durations noted.
Triage categories include emergency (referred to specific location), urgent (scheduled same day), non-urgent (scheduled within 48 hours), and routine (scheduled next available). Document the recommendation provided and client response - whether they accepted, declined to monitor, will seek second opinion, or other responses.
Pro-tip: Use checkbox fields for common symptoms to speed documentation and ensure consistency.
Note whether follow-up is required and when. This documentation serves multiple purposes: liability protection, quality assurance, and operational tracking of triage patterns.
Service level agreements that balance access with safety
SLAs for teletriage need careful calibration. Too aggressive and you promise more than you can deliver. Too conservative and clients seek care elsewhere.
Response time SLAs that work include immediate transfer to vet or emergency clinic direction for emergency symptoms, callback within 15 minutes if vet consultation needed for urgent symptoms, callback within 2 hours during business hours for non-urgent cases, and response by 9am next business day for after-hours messages.
Documentation SLAs include triage form completed during call, full notes entered in practice management system within 1 hour, emergency referrals documented immediately, and quality review of triage decisions within 24 hours.
These SLAs create accountability without overwhelming your team. They also set clear client expectations about response times.
The veterinarian callback threshold matrix
Not every case needs immediate veterinarian involvement, but clear thresholds prevent receptionists from making medical decisions beyond their scope.
| Symptom Category | Receptionist Can Handle | Requires Vet Callback |
|---|---|---|
| Single vomit episode, acting normal | Schedule appointment | N/A |
| Multiple vomiting episodes | Gather information | Determine urgency |
| Bloody vomit | Direct to emergency | Immediate if questioning |
| Minor wound, no bleeding | Schedule appointment | N/A |
| Active bleeding | First aid instructions + emergency referral | If client hesitant |
| Difficulty breathing | Immediate emergency referral | N/A |
| Limping, weight bearing | Schedule appointment | N/A |
| Limping, no weight bearing | Gather information | Assess need for immediate care |
| Known chronic condition flare-up | Check recent records, schedule | If symptoms differ from usual |
| Suspected toxin ingestion | Immediate emergency referral | If specific toxin questions |
This matrix removes guesswork while keeping veterinarians focused on cases requiring medical judgment.
Remote monitoring versus in-clinic decision rules
The hardest teletriage decisions involve borderline cases where remote monitoring might be appropriate but carries risk. Clear decision rules help staff navigate these situations.
Cases safe for remote monitoring with specific instructions include single vomit episode in otherwise healthy adult dog, soft stool without blood in adult animals, minor scrapes without puncture wounds, mild eye discharge without squinting, and occasional coughing without breathing changes.
Cases requiring in-clinic evaluation include any symptom in pets under 6 months or over 10 years, multiple symptoms occurring together, progressive worsening over 24 hours, any symptom in pets with chronic conditions, and behavioral changes lasting over 48 hours.
Client monitoring instructions should specify timeframes and warning signs. "Based on what you've described, monitoring at home for the next [timeframe] is reasonable. However, please bring [pet name] in immediately if you notice symptoms worsening or not improving within [timeframe], new symptoms developing, or [specific warning signs for their situation]."
Tell clients to keep track of symptom frequency, changes in eating/drinking, energy level and behavior, and urination and bowel movements. Always emphasize they can call back with concerns or questions and that reassessment is always available. This framework gives clients clear parameters while maintaining safety boundaries.
Managing after-hours triage within VCPR constraints
After-hours triage presents unique challenges. You can't examine patients, established clients expect some guidance, and emergency clinics may be far away or expensive.
A structured after-hours voicemail system works well: "If your pet is experiencing [list emergency symptoms], please proceed immediately to [emergency clinic name and address]. For other concerns, please leave a detailed message including your pet's symptoms and when they started, whether your pet is eating, drinking, and eliminating normally, and any medications or treatments you've given. We'll return your call by 9am. If symptoms worsen, don't wait - seek emergency care."
Some clinics offer limited after-hours triage through on-call services. This requires even stricter protocols including only established clients (active VCPR within 12 months), clear documentation of limitations discussed, no new prescriptions or treatment changes, emergency referral for anything beyond minor issues, and mandatory follow-up scheduling for next business day.
Quality control: Reviewing triage decisions for consistency
Regular audits of triage decisions identify training gaps and liability risks before they become problems.
Weekly triage audit should include random sample of 10 triage calls, check documentation completeness, verify appropriate urgency classification, confirm protocol adherence, review client outcomes if available, and identify patterns in mistakes or hesitation.
Track metrics like percentage of emergency referrals that were admitted (should be high), same-day appointments that could have waited (should be low), and callbacks requesting earlier appointments (indicates under-triaging).
When you spot patterns, address them through targeted training rather than broad policy changes. If receptionists consistently under-triage breathing issues, run a focused respiratory emergency training. If they over-triage skin conditions, review dermatology basics.
Integrating teletriage data with practice operations
Your teletriage workflow generates valuable operational data. Which symptoms drive most emergency referrals? When do triage calls peak? How many could be handled through better client education?
Clinics use this information to adjust staffing, create client resources, and identify service gaps. Multiple weekly urinary blockage referrals might indicate need for extended hours. Anxiety-related calls spiking during thunderstorm season suggests opportunities for proactive client communication.
Modern practice management platforms can track triage patterns automatically, flagging trends and generating reports. This transforms teletriage from a necessary evil into strategic intelligence about client needs and practice opportunities. Some clinics even use triage data to identify candidates for telemedicine services, chronic care management programs, or preventive care outreach.
The same systems managing liability risk become tools for practice growth.
Building staff confidence through scenario training
The best protocols fail if staff don't trust them. Regular scenario training builds confidence and identifies gaps in your scripts.
Run monthly triage drills where staff practice handling common situations:
-
Suspected bloat in a large breed dog
-
Cat straining in litter box
-
Puppy ate chocolate 30 minutes ago
-
Senior dog suddenly can't stand
-
Client angry about wait time for non-emergency
Record these sessions (with permission) and review as a team. You'll quickly spot where scripts need refinement or where individual staff need support.
Consider creating a "triage champion" role - someone who becomes the go-to resource for questions and maintains protocol documentation. This person can identify when updates are needed and ensure consistency across shifts.
The real cost of unstructured teletriage
Clinics without structured teletriage systems face hidden costs beyond liability risk. Inconsistent advice frustrates clients who get different answers from different staff members. Veterinarians waste time returning calls that receptionists could have handled. Emergency clinics stop referring cases back when they repeatedly see inappropriate referrals.
Staff stress skyrockets when every phone call requires judgment calls without clear guidelines. Receptionists burn out from constantly worrying they gave wrong advice. The whole team spends mental energy on decisions that should be automatic.
One clinic tracked their triage-related time before and after implementing structured protocols. Before: veterinarians spent roughly 90 minutes daily on callbacks, receptionists averaged 15 minutes per triage call, and documentation happened sporadically. After: vet callbacks dropped to 30 minutes, triage calls averaged 8 minutes, and documentation compliance hit 95%.
Technology's role in scaling safe teletriage
While protocols and training form the foundation, technology multiplies their effectiveness. AI-powered operational software can guide receptionists through triage scripts, automatically document responses, and flag cases requiring immediate veterinarian review.
These platforms work by codifying your protocols into interactive workflows. As receptionists ask questions, the system suggests next steps based on responses. Documentation happens automatically. Urgency classifications follow your predetermined rules. The result is consistent triage regardless of who answers the phone.
The best systems also learn from outcomes, identifying patterns in successful versus problematic triage decisions. They can alert management to staff members struggling with specific situation types or highlight when protocols need updating based on changing practice patterns.
This isn't about replacing human judgment - it's about supporting staff with tools that reduce cognitive load and ensure consistency. Your experienced receptionists still apply situational awareness and empathy. They just don't have to remember every protocol detail or worry about documentation while managing distressed clients.
Moving from reactive to proactive triage
Teletriage doesn't have to be a liability nightmare. With structured scripts, clear thresholds, and proper documentation, it becomes a valuable service that improves patient outcomes while protecting your practice.
Start simple. Pick five common scenarios and create basic scripts. Test them for a month. Refine based on what you learn. Gradually expand coverage as staff confidence grows.
Perfect protocols don't exist. You're aiming for consistency and safety, not eliminating all risk. Regular reviews and updates keep your system aligned with practice reality and regulatory requirements.
The clinics that master teletriage don't just reduce liability - they build client trust through consistent, professional responses to pet health concerns. In a world where clients increasingly expect immediate answers, structured teletriage becomes a competitive advantage that sets professional practices apart from those hoping good intentions are enough.
Teletriage doesn't have to be a liability nightmare. With structured scripts, clear thresholds, and proper documentation, it becomes a valuable service that improves patient outcomes while protecting your practice.
Start simple. Pick five common scenarios and create basic scripts. Test them for a month. Refine based on what you learn. Gradually expand coverage as staff confidence grows.
Ready to elevate your clinic’s efficiency?
Join 500+ veterinary clinics using Veterinaryly to save time, reduce administrative overhead, and improve patient care.