

That sinking feeling when a post-op patient crashes three hours after what seemed like a routine spay? Or when the overnight tech calls at 2 AM because they can't figure out what anesthesia protocol was used? These aren't random events—they're predictable results of documentation gaps that exist in almost every veterinary clinic.
The real killer isn't the surgery itself. It's the handoff between shifts, the missing consent checkbox that should've flagged a heart condition, or the recovery instructions that somehow got sent to the wrong client. After building operational systems for dozens of veterinary clinics, the pattern is clear: perioperative complications track directly back to specific documentation failures during transitions.
Most clinics think they have this covered with practice management software and paper forms. They don't. Not even close.
The Three-Hour Window Where Everything Falls Apart
Morning tech preps eight surgeries, scribbling notes on whiteboards, sticky notes, maybe entering some details into the computer. The surgeon moves through cases, making mental notes—this one needed extra ketamine, that one had unexpected bleeding, another had a reaction to the pre-med.
By 2 PM, morning tech has left, taking all that context with them. Afternoon recovery tech inherits eight patients with minimal handoff notes. Flying blind.
This is where patients die. Not from surgical complications, but from missed information during shift changes.
A French Bulldog was lost at one clinic last year because nobody documented early signs of brachycephalic airway syndrome during induction. Recovery tech didn't know to watch for respiratory distress. By the time they noticed labored breathing, it was too late. Documentation just said "routine neuter, no complications."
That's not isolated. It's systematic failure that plays out differently every week across thousands of clinics.
Why Your Current Documentation System Is Fiction
Average clinic uses between 4-7 different documentation points for a single surgery. Paper consent forms, digital patient records, anesthesia monitoring sheets, whiteboard schedules, verbal handoffs, discharge instructions, follow-up reminders.
Never miss a pet’s appointment again.
Veterinaryly helps you schedule, confirm, and manage every appointment and patient record effortlessly.
- Centralized appointment & patient management
- Automated client reminders
- Staff scheduling & task tracking
No credit card required
None of these talk to each other. Information gets transcribed, translated, summarized, and lost at every step. By the time complications develop, critical details that could've prevented them are scattered across multiple systems—if they were captured at all.
One clinic I worked with discovered they were using three different consent forms depending on which tech was working. Another had anesthesia protocols that existed only in their senior surgery tech's head—when she went on maternity leave, complication rates jumped 40%.
Everyone knows the system is broken, but they're too busy putting out fires to fix it.
The Consent Form That's Setting You Up for Lawsuits
Standard consent forms are legal protection theater. They cover the clinic's liability but miss operational details that actually prevent complications.
Real example: Client signed standard surgical consent for dental cleaning. Buried in the client's intake paperwork from two years ago was a note about previous adverse reaction to acepromazine. Consent form didn't prompt anyone to check for drug reactions. Dog went into cardiac arrest during pre-medication.
Lawsuit wasn't about whether client consented to anesthesia risks. It was about the clinic's failure to have a systematic way to surface critical historical information at the point of care.
Most consent processes miss key details. They don't force documentation of previous anesthetic events and reactions, current medications including supplements, specific monitoring requirements based on breed/age/condition, clear escalation triggers and thresholds, or who specifically is responsible for which monitoring parameters.
They don't connect to your anesthesia protocols. Person getting consent rarely talks to person administering drugs. Form sits in folder while actual decisions happen in isolation.
They don't create actionable flags. Even if someone writes "sensitive to sedation" on a form, there's no systematic way to ensure the anesthetist sees it, understands what it means, and adjusts protocols accordingly.
Anesthesia Records That Nobody Actually Reads
Walk into any surgery suite and you'll see anesthesia monitoring sheets covered in tiny boxes, filled with numbers that nobody looks at after the patient wakes up. Heart rate: 68, 72, 70, 74. Respiratory rate: 12, 14, 12, 13. Rows of data that mean nothing in isolation.
What actually matters for handoffs and recovery isn't the raw numbers—it's the patterns and exceptions. Did heart rate drop when you pushed propofol? Did you need to bump up iso halfway through? Was there excessive bleeding that might affect recovery?
Traditional anesthesia records capture data but not decisions. They show what happened but not why it matters.
Recovery tech getting a patient needs to know this patient required 30% more iso than typical for their weight, blood pressure dropped twice but responded to fluid bolus, took longer than expected to intubate due to small trachea, and is currently stable but needs monitoring for respiratory depression.
Instead, they get a sheet of numbers and "stable throughout procedure."
The Handoff That Happens in Hallways
Shift changes in veterinary clinics are where information dies. Morning tech has eight patients to hand off, five minutes to do it, and afternoon tech is already dealing with a walk-in emergency.
"Room 2 is a spay, routine, nothing special. Room 3 is the dental, pulled four teeth, seems good. Room 4 is the neuter, he's a little slow to wake up but probably fine..."
That "probably fine" patient? He had a difficult intubation, required atropine during surgery, and his owner mentioned this morning that he seemed lethargic yesterday. None of that makes it into the five-second verbal handoff.
Real handoffs in busy clinics average under 30 seconds per patient. Critical details get compressed into "doing well" or "watch this one." Receiving tech has no structured way to know what specifically to watch for or when to escalate concerns.
Information that gets lost includes specific anesthesia adjustments and why they were made, subtle changes in vital sign patterns, owner concerns mentioned during drop-off, medications given and when, expected vs actual recovery timeline, and specific monitoring parameters for that patient.
Without structured handoff documentation, every shift change is a gamble.
Post-Op Messages That Create More Problems
Collect all the post-op instruction sheets your clinic has sent out in the last month. You'll find multiple versions of the same procedure, conflicting instructions between different vets, generic templates that don't match what actually happened, and critical information buried in paragraph 3 of page 2.
Clients get these novels of instructions, panic about everything, and call back about the wrong things while missing actual warning signs.
One clinic tracked their post-op callbacks. 73% were about normal healing that clients thought was abnormal. Meanwhile, they had two serious complications where clients didn't call because the symptoms weren't specifically mentioned in their instructions.
Handing clients a printed sheet and hoping for the best doesn't work. Clients are stressed, their pet is groggy, and they're juggling carriers and credit cards and discharge conversations. They're not absorbing anything.
Predictable outcome: They get home, pet does something weird, they panic, they call. Or worse—pet does something concerning, they assume it's normal, they don't call.
The Hidden Cost of Bad Documentation
Average cost of a surgical complication requiring additional treatment: $1,800-3,500. Average settlement for a documentation-related malpractice claim: $15,000-45,000. Staff time spent on preventable post-op callbacks: 2-3 hours daily. Client trust lost after a preventable complication: immeasurable.
| Issue | Cost/Impact |
|---|---|
| Average cost of a surgical complication requiring additional treatment | $1,800-3,500 |
| Average settlement for a documentation-related malpractice claim | $15,000-45,000 |
| Staff time spent on preventable post-op callbacks | 2-3 hours daily |
| Client trust lost after a preventable complication | immeasurable |
One mid-sized clinic was losing roughly $8,000 monthly to documentation-related inefficiencies. Not from major lawsuits or deaths—just from daily friction of callbacks, repeated work, miscommunications, and minor complications that required follow-up care.
They had three techs spending 40% of their time dealing with issues that proper documentation would have prevented. That's one and a half full-time salaries going to damage control instead of patient care.
Building Documentation That Actually Works
Real perioperative documentation isn't about covering legal bases—it's about creating information flow that prevents problems before they happen.
Start with your consent process. Stop using generic forms that clients sign without reading. Create dynamic consent workflows that pull forward all historical reactions and complications, force documentation of specific risk factors, generate automatic flags for the surgical team, create clear monitoring parameters based on patient specifics, and document who is responsible for what.
Your anesthesia records need to capture decisions, not just data. Instead of recording heart rate every 5 minutes, document when and why protocols were adjusted, how the patient responded to each drug, any unexpected responses or requirements, and specific recovery concerns based on what happened.
For handoffs, implement structured documentation that takes 2 minutes but covers what was expected vs what actually happened, specific parameters to monitor, clear escalation triggers, medications given with exact times, and owner concerns or comments from drop-off.
-
Immediate discharge
What to expect in next 4 hours
-
Evening check-in
Automated text with 3 specific things to monitor
-
Next day follow-up
Targeted questions about actual recovery
-
48-hour checkpoint
Confirmation of normal healing
This isn't about more documentation—it's about the right documentation at the right time.
The Workflow That Prevents Complications
Information flow through a surgical case follows this pattern:
Pre-Surgery Day: Client books surgery → System automatically sends pre-op instructions → Client completes detailed health update form online → Responses generate specific flags and requirements
Surgery Morning: Check-in tech reviews flags → Documents any new concerns → Creates patient-specific monitoring plan → Handoff to surgery team includes all context
During Surgery: Real-time documentation of decisions and adjustments → Photo documentation of any findings → Continuous update of recovery requirements → Automatic alert generation for specific parameters
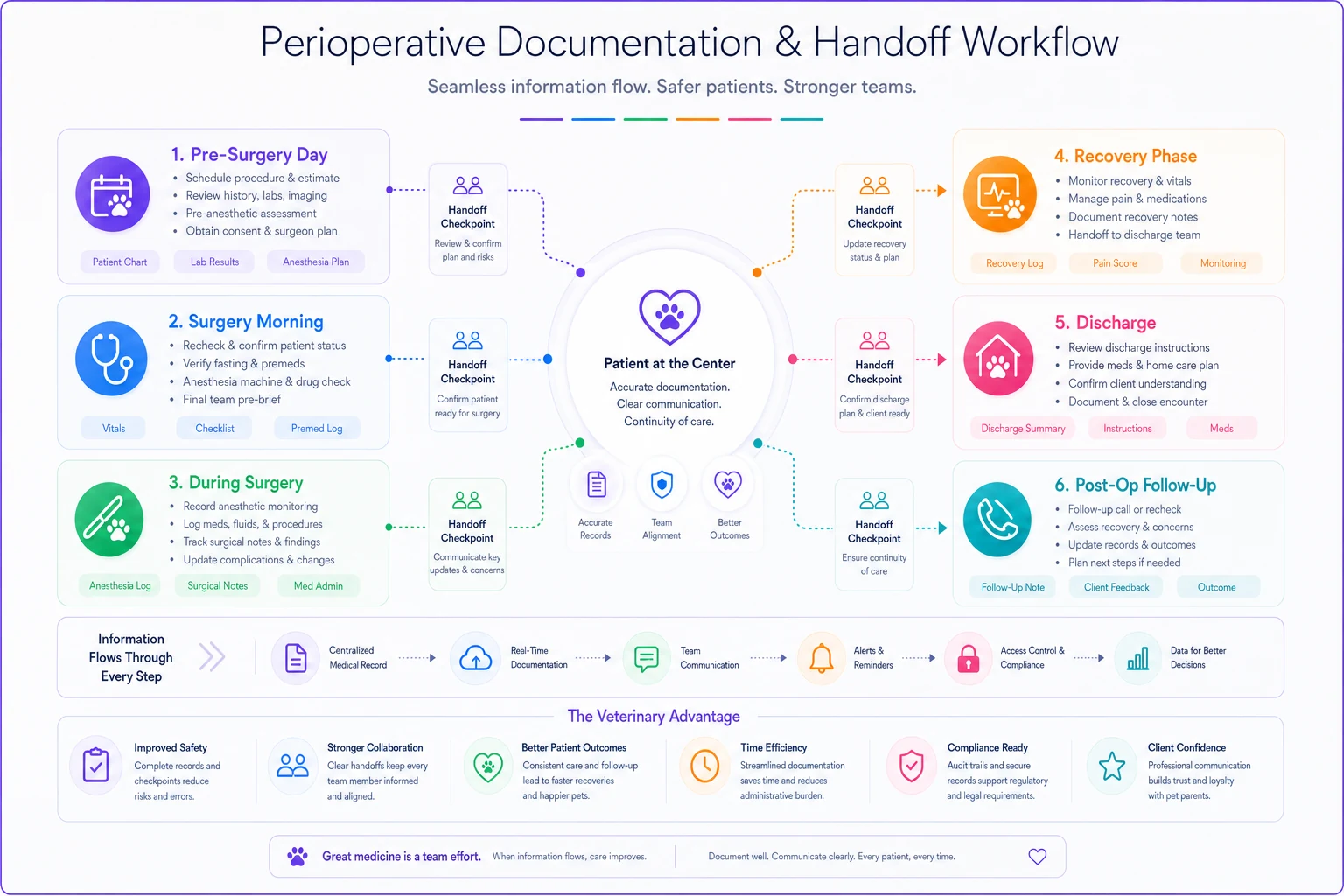
Here's a quick visual of that workflow.
Recovery Phase: Structured handoff with all context → Clear monitoring checklist with thresholds → Automated escalation if parameters exceeded → Documented decision trail for all interventions
Discharge: Customized instructions based on actual procedure → Staged follow-up messages → Automated check-ins with specific questions → Clear re-check scheduling if needed
Post-Op Period: Automated wellness checks → Client response tracking → Immediate flag for concerning responses → Documented follow-up trail
This isn't about more documentation—it's about the right documentation at the right time.
Why Templates Alone Won't Save You
Beautiful templates mean nothing if they're not integrated into actual workflows. Clinics with gorgeous consent forms that nobody fills out properly, detailed handoff checklists that get ignored during busy periods, and comprehensive post-op instructions that never match what actually happened during surgery.
Problem isn't the templates—it's the system. Or lack thereof.
Templates work when they're integrated into existing workflows, not added on top, automatically populated with relevant information, impossible to skip or shortcut, connected to downstream processes, and actually used to drive decisions.
A consent form that doesn't automatically flag the anesthetist about a previous reaction is just paper. A handoff checklist that doesn't get filled out during shift change is fiction. Post-op instructions that aren't customized to what actually happened are noise.
The Role of Automation in Preventing Human Error
AI-powered operational software becomes critical here—not as fancy add-on, but as the backbone that makes good documentation actually happen. When you're dealing with 15-20 surgeries a day across multiple doctors and rotating staff, human memory and manual processes will fail. Every single time.
Modern AI automation can pull historical data into consent forms automatically, flag unusual patterns in monitoring data, generate customized discharge instructions based on actual procedure notes, and trigger follow-up messages at exactly the right intervals. It's not about replacing clinical judgment—it's about ensuring critical information never gets lost in the chaos of daily operations.
Clinics with lowest complication rates aren't necessarily the ones with the best surgeons. They're the ones with systems that ensure every piece of critical information makes it to the right person at the right time, every time.
When This Actually Matters (And When It's Overkill)
Not every clinic needs comprehensive perioperative documentation systems. If you're doing three surgeries a week with the same team every day, you might be fine with your current approach.
But if you have multiple doctors with different protocols, rotating surgical teams, shift changes during recovery periods, more than 10 surgeries per day, any staff turnover, or plans to scale or add locations, then documentation gaps will eventually hurt you. Not a matter of if, but when.
The question isn't whether you need better documentation—it's whether you'll implement it before or after a preventable tragedy.
Real Implementation: Starting Tomorrow
You don't need to overhaul everything at once. Start with your highest-risk gap. For most clinics, that's the handoff between surgery and recovery.
Tomorrow morning, implement one structured handoff document that captures what drugs were given and when, any protocol deviations and why, specific monitoring requirements, clear escalation triggers, and owner concerns from drop-off.
Use it for one week. Track how many questions the recovery team has to ask. Count the callbacks. Monitor complications.
Then expand to your next gap. Maybe consent forms that actually capture relevant history. Or post-op messaging that prevents panic calls.
Build your system incrementally, but build it deliberately.
The Bottom Line on Perioperative Documentation
Every surgical complication that stems from missing information is preventable. Every callback about normal healing that wasn't properly explained is waste. Every handoff that loses critical context is a gamble.
The gap between pre-op and recovery isn't a clinical challenge—it's an operational one. Clinics that get this right aren't necessarily more skilled. They're more systematic.
Your surgical outcomes are only as good as your weakest documentation link. In most clinics, that's not a weak link—it's a missing chain entirely.
Tools exist to fix this. AI-powered platforms can automate the capture, flow, and delivery of critical information throughout the perioperative period. The question isn't whether you need better documentation systems. It's whether you'll implement them proactively or reactively.
Because eventually, every clinic faces the patient that crashes because somebody, somewhere, didn't document something important. The only choice is whether you'll be explaining why your systems failed, or confident they worked exactly as designed.
Ready to elevate your clinic’s efficiency?
Join 500+ veterinary clinics using Veterinaryly to save time, reduce administrative overhead, and improve patient care.